Stay Awesome
Injection Technique
Know exactly what we should be doing and WHY


What is wrong in the above picture?
Background:
This is my mother's arm.
She had been given four vaccines:
On the left she had Flu and COVID.
On the right (pictured) she had pneumococcal at the top, and Shingles at the bottom (from what I could glean as she recounted the tale).
The nurse giving the vaccine was training someone up. My mother heard her say to the trainee nurse "because we have got two to give in the same arm we have to leave a massive gap".
Is this right? What interval would YOU recommend? Can you find the answer in chapter 4 of the Green Book?
Anyway, this rationale clearly meant the second (shingles) vaccine was administered too low. It doesn't look like the deltoid to me. What do you think?
It also could have been given too shallow, OR the needle wasn't changed after drawing up, given the local reaction...
When we administer vaccines incorrectly there are several consequences in a situation like this:
Patient suffering. Let's face it. Its hard enough being stabbed in the arm CORRECTLY.
Vaccine hesitancy. My mum threatened to never have a vaccine again after this. Fortunately she's not allowed to commit to that, because her daughter is an immunisation enthusiast, and has to set a good example.
Reduced medicinal action. Will her vaccine be effective now? Too low and too shallow may lead to a suboptimal response.
Legal issues. This nurse possibly accidentally did an 'off-label' S/C administration of a drug which was not positioned in the deltoid muscle (where most vaccines hold their licence for). I only say 'possibly' because I don't know what her PGD specified.
Wasted clinic time. Incident reports, write ups, repeat appointments for review, complaints management....
Wasted money. Did you know Shingrix (although this case was using Zostavax) is over £200 per dose privately? Expensive mistakes if you draw up or administer incorrectly and have to repeat a dose.
Hesitancy is contagious. My mum obviously showed all her mates to get lots of sympathy. I wonder how many of them at the same village surgery opted out of a shingles jab after hearing about this? (We did have some words about being vaccine-positive around mates because I was worried about this)
Dis-reputing the profession. The NMC has very firm views about nurses not making the profession look bad. Check out the tribunal notes for this struck-off nurse
So, we have to be really really sure we are doing things correctly. It's mega sad when a vaccine gets the blame for 'not working' when it is actually more to do with how it was given. And we DO NOT want to harm our patients when we are trying to do EXACTLY THE OPPOSITE!
The Green Book (chapter 4) has all the guidance we need about how and where to administer, and what with. So, I'll leave that to the Green book to inform you further if you want to know more. However, here's some useful and novel stuff for you to have a browse of and don't forget to try the quiz at the bottom (when you have finished admiring the excellent deltoid muscles in the picture below!):
Which Arm Gets Vaccinated Could Matter More Than You Think, BUT the evidence is divided....
Could swapping arms in multi-dose schedules improve immune response? .
VIDEO - injection landmarking (scroll down)
BLOG - really picky injection technique debates (you might notice a familiar author of this one)
and this one... BLOG Ten tips for dealing with appointments that involve injecting children
Video: AMERICAN but useful to watch for advice on multidose vial management (note UK sometimes have different rules about alcohol swabs! Follow manufacturer instructions and local and UK policy -always) - also embedded below.
Should we use alcohol swabs before giving injections? A look at the arguments. (another familiar author)

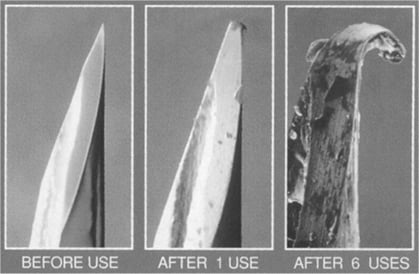
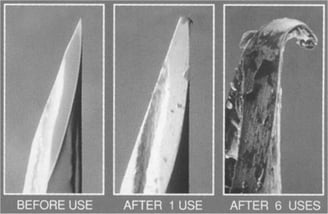
Ever seen a used needle under a microscope? You have now! THIS is a good reason why we should always change needles that have been used to draw something up.
Webinar (presented by yours truly)
Injection Perfection: Could Small Changes Improve Your Practice?

